 |
Research Article
Epidemiological surveillance and burden of serological infectious markers among adult population of New Juaben Municipality: A 6-year laboratory review from the Eastern Regional Hospital, Ghana
1 Faculty of Health and Allied Sciences, Koforidua Technical University, Koforidua, Eastern Region, Ghana
2 Department of Medical Laboratory Sciences, School of Allied Health Sciences, University of Health and Allied Sciences, Ho, Ghana
3 Department of Medical Laboratory, Eastern Regional Hospital, Koforidua, Eastern Region, Ghana
Address correspondence to:
Francis Abeku Ussher
Koforidua Technical University, Koforidua,
Ghana
Message to Corresponding Author
Article ID: 100074Z02FU2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ussher FA, Taufik O, Osei-Yeboah J, Lokpo SY, Danquah GD, Kwakye GK, Der J. Epidemiological surveillance and burden of serological infectious markers among adult population of New Juaben Municipality: A 6-year laboratory review from the Eastern Regional Hospital, Ghana. Int J Blood Transfus Immunohematol 2022;12(2):1–11.ABSTRACT
Aims: The study aimed at determining the epidemiological feature and burden of infectious markers among asymptomatic adult population in Koforidua.
Methods: This is a hospital-based retrospective study conducted at the Eastern Regional Hospital and comprised of a review of secondary data of prospective blood donors who visited the facility blood bank from January 2015 to December 2020. Archived data of 22,648 prospective blood donors comprising gender, age, and residential locations as well as results of infectious markers [syphilis, hepatitis C virus (HCV), hepatitis B virus (HBV), and human immunodeficiency virus (HIV)] were retrieved from the blood bank. Prospective blood donors were screened for infectious markers using rapid diagnostic test (RDT) kits. Hepatitis B, hepatitis C, and syphilis were screened using Abon, Micropoint, Just check, Green life, and Accurate rapid diagnostic test kits whereas HIV was screened using First response kits.
Results: The overall cumulative crude prevalence rate of blood-borne pathogens was 69.76 per 10,000, 27.45 per 10,000, 115.15 per 10,000, and 33.87 per 10,000 population for HBV, HCV, syphilis, and HIV, respectively. A prominent year-on-year decreasing trend of hepatitis B viral infection and HIV was observed in the general population. On the other hand, syphilis infection recorded an increasing trend of infection while HCV infection demonstrated a dual trend with a decrease from 2016 to 2018 and an increase till the end of 2020.
Conclusion: The overall burden of transfusion transmissible infections (TTIs) was high among the populace with a prominent male gender preponderance. The rates of the infections were highly marked among the youth population within the ages of 20 to 29 years.
Keywords: Blood donors, Crude prevalence, Transfusion transmissible infection
Introduction
Medical demand for blood and blood products has risen dramatically across sub-Saharan Africa due to rapid improvements in healthcare and a rise in the number of attendants for surgical treatment due to the scaling up of surgical technologies [1]. However, countries within the region have persistent blood product shortages at both regional and national levels [2]. This has resulted in insufficient access to healthy and safe blood and blood product supplies in health centers and remains a significant public health issue across the African sub-regions [3]. Blood transfusion is a therapeutic intervention in modern medicine that cuts across several clinical disciplines, saving millions of lives yearly [2],[4]. This hematological supportive intervention is a phenomenon driven by many overarching factors, including endemicity of infections related to anemia, blood loss linked to accidents, high incidence of sickle cell anemia, medical and obstetrical emergencies, and malnutrition, among others [3]. The procedure is not without risk, with risks ranging from possibly lethal immunohypersensitivity reactions to the possibility of blood-borne pathogen transmission from donor to the recipient [1]. The morbidity and mortality resulting from contaminated blood transfusions have far-reaching consequences for the patients and their families, societies, and the community at large [4],[5]. Prolonged and untreated blood-borne infections may result in pathologies such as cirrhosis, liver fibrosis, hepatocellular carcinoma (HCC), end-stage liver disease, and mortality due to hepatic disease, as well as a weakened immune system that paves the way for life-threatening opportunistic infections [6]. Hepatitis B virus (HBV), hepatitis C virus (HCV), human immunodeficiency virus (HIV), and syphilis are the principal blood-borne pathogens present in blood [7]. These microbial agents are the most critical pathogenic agents mainly implicated in transfusion-transmitted infections (TTIs) and continue to be a global public health problem [7]. It is estimated that 350 million people have chronic HBV infection, 170 million have HCV infection, and 38 million people have HIV infection [8]. In Eastern Ghana, Lokpo et al., 2017 reported a seroprevalence of 4.06%, 7.23%, 5.81%, and 10.42% for HIV, HBV, HCV, and syphilis, respectively among blood donor population in Akwatia. A similar study from the region also recorded a prevalence of 4.5% for HIV, 13.2% for HBV, 8.0% for HCV, and 15.3% for syphilis among blood donors in Koforidua [9].
Although the problem of unsafe blood transfusion perpetuates in most developing countries, including Ghana, most health facilities in the country use blood transfusion as part of their life-saving procedures [10]. Hence the issue of blood transfusion requires immediate attention [11]. Moreover, there is a scarcity of data on the prevalence of the blood-borne pathogens infection in the New Juaben District of Eastern Ghana. With this background, the current study focused on determining the epidemiological feature and burden of infectious serological markers among the adult population in the New Juaben Municipality.
MATERIALS AND METHODS
Study design
This study is a hospital-based retrospective study conducted at the Eastern Regional Hospital and comprised of a review of secondary data of prospective blood donors who visited the facility blood bank from January 2015 to December 2020.
Study site description
This study was conducted in the Eastern Regional Hospital in Koforidua which is within the New Juaben South Municipality. The New Juaben South Municipality is one of the 260 Metropolitan in Ghana and forms part of the thirty-three (33) municipalities and Districts in the Eastern Region. It was established in 1988 by the legislative Instrument (LI) 1426 and lies between longitude 1030’ West and 0030’ East and Latitudes 60 and 70 North with Koforidua as its capital. The municipality shares common boundaries with East-Akim Municipal to the North-East, Akwapim North Municipal to the East and South, and Suhum Municipal to the East. It covers a land area of 159 square kilometers representing approximately 0.6% of the total surface area of the Eastern Region (Ghana Districts.Com).
The Eastern Regional Hospital (ERH) is the Regional Hospital in Koforidua, the capital of the Eastern Region of Ghana. It provides a range of services to the local (and extended rural) population. These include providing specialist care in visceral surgery, pediatric surgery, obstetrics and gynecology, neonatology and pediatrics, dermatology, venereology, and HIV medicine and laboratory medicine. The ERH is a 400-bed complement hospital with 50 doctors. In addition to offering clinical care to inhabitants of Koforidua and its surrounding districts, it also serves as a referral hospital.
Data analysis
Data was entered into the Microsoft Office Excel 2016 spreadsheet. Descriptive and inferential analysis were done using IBM Statistical Package for the Social Sciences (SPSS Inc., Chicago, USA) (www.spss.com) version 25.0 to estimate the crude prevalence rate, the direct age-standardized rate, and trend of blood-borne infections in the general population. The present study used prospective blood donors aged between 17 and 58 years who visited the Eastern Regional Hospital during the six years (2015–2020) as a proxy population and published population of the district as the base population [12].
Data collection
The study included male and female blood donors aged between 17 and 58 years whose complete records were available for review. The blood donor group was a family/replacement blood donor group and comprised of repeated donors (majority) and first-time donors. Demographic parameters included age, gender, and residential location. Results of infectious markers (HIV, HBV, HCV, and syphilis) screening using rapid diagnostic test kits from a total of 22,648 blood donors were obtained from the archives at the blood bank.
Ethical consideration
According to the Ghana Health Service (GHS) Ethics Review Committee standard operating procedures, “research categories that are eligible for exempt review include: research involving the use of educational tests (cognitive, diagnostics, aptitude, and achievement), survey procedures, interview procedures, or observation of public behavior. Unless: (i) information obtained is recorded in such a manner that human subjects can be identified, directly or through identifies linked to the subjects, and (ii) any disclosure of the human subjects’ responses outside the research could reasonably place the subjects at risk of criminal or civil liability or be damaging to the subjects’ financial standing, employability, or reputation or place the subject at risk for loss of insurability.” This study posed minimum risk to participants as no personal identifiers were collected or stored. However, written approval from the Eastern Regional Hospital was obtained to carry out the study in the facility. Analysis of the data was anonymous and non-linked. Blood donor identification numbers were used for processing the testing of the individual participants. Patient’s data and information were held confidential and used for academic purposes only.
RESULTS
In this study, the mean age of the male participants was 25.05±7.05 while that of the female participants was 27.14±7.49 (see Table 1).
Overall prevalence of TTIs in New Juaben Municipality
The cumulative crude prevalence rate of transfusion transmissible infections (TTIs) stood at 246 per 10,000. Within the six years under review, it was observed that syphilis infection was the most prevalent infection among the residents of New Juaben Municipality with a crude rate of 115.15 per 10,000 population, whereas HCV was the least observed infection with an overall rate of 27.45 per 10,000 population (see Table 2).
Age and gender distribution of HBV infection in New Juaben Municipality
Within the six year-period under review, the overall crude prevalence of hepatitis B viral infection stood at 135.35 per 10,000 persons for the male population and 7.12 per 10,000 persons among the female population. Age-standardized rates of 135.42 and 7.18 per 10,000 persons were recorded among male and female populations, respectively. Irrespective of the gender, the overall highest case density was recoded among the populace within the age brackets of 20–29 years with a cumulative crude rate of 202.49 per 10,000 population. In general, the review observed a significant decreasing burden of hepatitis B viral infection with an increasing age group among both the males and females population except <20 age group, which buck the trend (see Table 3).
Age and gender distribution of HCV in New Juaben Municipality
The review observed overall HCV crude rates of 1.86 and 55.05 per 10,000 persons for the female and male populations respectively. The age-standardized rate of 54.12 per 10,000 persons was recorded among the male population, while 1.91 per 10,000 persons was observed among the female population. The age group of <20 years (78.23 per 10,000) and 20 to 29 (79.79 per 10,000) recorded the highest overall case density of HCV regardless of the gender. Except for the age group <20, the review showed an inversely proportional burden of hepatitis C viral infection with an increasing age group among both males and females population (see Table 4).
Age and gender distribution of syphilis in New Juaben Municipality
The overall crude rates of syphilis infection observed within the years under review were 229.71 and 8.98 per 10,000 persons among the male and female populations respectively. The age-standardized rates recorded in the study were 227.37 and 9.06 per 10,000 persons for male and female populations, respectively. The age bracket of 20–29 years recorded the overall highest syphilis infection rate with a cumulative 304.50 per 10,000 population. Regardless of the gender, the review observed a significant decreasing incidence of syphilis infection with increasing age from 20–29 years and above (see Table 5).
Age and gender distribution of HIV in New Juaben Municipality
The overall crude rates of HIV infection recorded in this study for the male and female populations were 64.93 and 5.08 per 10,000 persons. Also, the age-standardized rates of 64.12 and 5.14 per 10,000 persons were observed for both the male and female population, respectively. Irrespective of the gender, individuals within the age brackets of 20–29 years recorded the highest HIV infection burden. An overall decreasing rate of HIV infection was observed from the age group of 20–29 years and above for both males and females population (see Table 6).
Year-on-year prevalence of infectious markers in New Juaben Municipality
The overall cumulative year-on-year analysis showed a prominent increasing trend of syphilis infection peaking in 2020 at 33.60 per 10,000 population. However, the trend analysis also revealed a reduction in the infection rate from 19.53 per 10,000 in 2015 to 11.70 per 10,000 in 2020 for HBV and from 11.08 per 10,000 in 2016 to 2.81 per 10,000 population at the end of 2020 (see Table 7).
Year-on-year gender variation of infectious markers in New Juaben Municipality
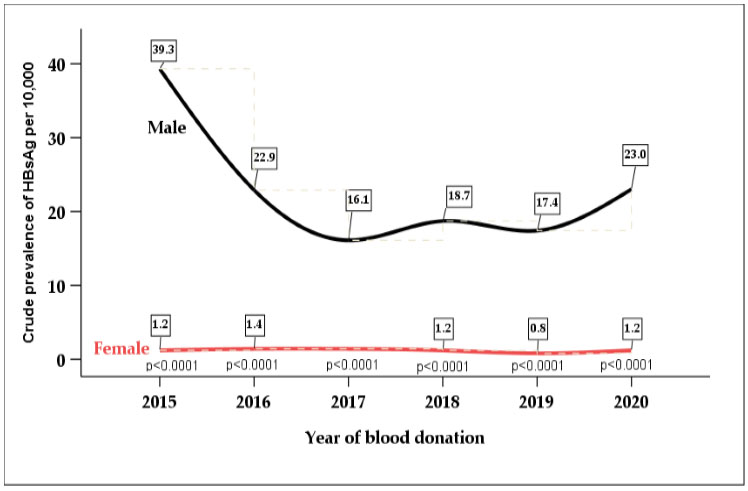
The year-on-year trend analysis for the 6-year under review revealed a steep decline in the overall hepatitis B viral infection burden among the male population from a peak year (2015) to 2017. It sparingly increased till the last review year (2020). A steady patty trend was observed for the female population throughout the review years. A prominent gender disparity with infection preponderance tilted toward the male population was observed for the entire 4-year period (see Figure 1).
The review observed a U-shape trend of HCV infection burden from 2016 to 2020 among the male population. A prominent gender variation was observed within the review period, with a higher burden of HCV infection occurring among the male group than their female counterparts year-on-year (see Figure 2).
The year-on-year trend showed an undulating movement of the overall syphilis infection burden among the male populace from 2015 through 2018 with a sharp increase in the crude rate in the last two review years, peaking in 2020. A steady patty trend was observed for the female population throughout the review years. A prominent gender variation was observed with male predominance compared to their female counterparts (see Figure 3).
The review observed a steep decreasing trend of HIV infection burden from a peak in 2016 and through in the fifth review year 2019 for the male population. In addition, a prominent gender disparity with infection preponderance tilted toward the male population was observed for the entire 6-year period under review (see Figure 4).










Discussion
In this study, a total of 22,648 prospective blood donors were screened and recorded at the Eastern Regional Hospital within the 6-year under review. The study observed male donor predominance compared to the females. This observation is consistent with previous studies conducted in different parts of the country [6],[13]. Although several previous studies have reported this gender bias among prospective blood donors, there are no substantial explanations for this regular occurrence of male dominance in the donor population among Ghanaians. However, an earlier report extrapolates that certain beliefs, socio-cultural practices, and male proactiveness in decision-making may be some of the factors influencing this recurring phenomenon [14]. Other reports also suggested that causes such as pregnancy, breastfeeding, a higher incidence of iron deficiency anemia in women, monthly blood loss via menstruation, and the widespread belief that men are healthier than women may be accountable for the female donor minority [1],[15]. In this study, the overall cumulative crude prevalence rate of blood-borne pathogens among the residents of the New Juaben Municipality was 69.76 per 10,000, 27.45 per 10,000, 115.15 per 10,000, and 33.87 per 10,000 population for HBV, HCV, syphilis, and HIV, respectively (Table 2). It is important to note that a direct comparison of our findings to similar studies conducted previously in Ghana and other West African countries was not possible because this is the first study of its kind in the country and one of the few in Africa. Earlier authors expressed their findings as percentages of reactive cases among donor populations rather than the incidence among the general population. Notwithstanding, an earlier study by Lokpo and colleagues [6] within the region recorded an overall seroprevalence of 4.06%, 7.23%, 5.81%, and 10.42% for HIV, HBV, HCV, and syphilis infections, respectively. In similar studies, Adu-Poku et al. [10] reported a relatively lower prevalence of HIV (3.9%), HBsAg (5.0%), HCV (4.2%), and syphilis (5.2%). In contrast, Nkrumah et al. [16] recorded relatively higher seroprevalences of 13.8% and 9.4% for HBsAg and HCV respectively among subpopulations of Ghanaians. The rate of these major TTIs also compares with earlier reports in other African countries by Nwankwo et al. [17] in Nigeria, Bisseye et al. [18] in Gabon and Jacques et al. [19] in Cameroon. However, the overall crude prevalence rate of the infectious markers observed in the current study is higher compared to the rates recorded by Khedmat et al. [20] [HBsAg (488 per 100,000), HCV (80 per 100,000), syphilis (5.5 per 100,000), and HIV (3.2 per 100,000 population)] and Mohammadali and Pourfathollah [21] [HBsAg (388 per 100,000), HCV (112 per 100,000), syphilis (10.5 per 100,000) and HIV (5.4 per 100,000 population]. Likewise, Steele et al. (2020) reported relatively lower rates of the three viral infections, HIV (2.59 per 100,000), HBsAg (6.32 per 100,000), and HCV (19.00 per 100,000) in the United States. Previous reports have postulated several attributable factors that may account for changes in the burden of blood-borne pathogens across different populations. The number of sexual partners, immunization status, sanitary conditions, education, social status, geographic location, and the sensitivity of the test kits used have all been proposed as primary determinants of the rate of transfusion transmissible infections [15],[22],[23]. In the same vein, factors such as tattooing, bloodletting exercises, cultural rituals like female genital mutilation, and donor selection criteria, among other things, have been proposed [6]. Of particular note is the finding of gender disparity in the rate of TTIs among the inhabitants of the New Juaben Municipality with male preponderance. It was observed that irrespective of the blood pathogen type, the crude prevalence rate showed an escalated prominent male gender predominance [137.35, 55.05, 229.71, and 64.93 per 10,000 population] compared to their female counterparts [7.12, 1.86, 8.98, and 5.08 per 10,000 population] for HBsAg, HCV, syphilis, and HIV, respectively. Our results add to a growing body of knowledge where male preponderance to blood-borne pathogens has been reported. The reason for this inconsistent infection pattern observed in the current study is not clear but could partly reflect the inequality in the recruitment of donors concerning gender. The males in this study outnumber their female counterparts; hence, the male populations estimated burden of blood-borne pathogens could be skewed. Notwithstanding, the male preponderance of transfusion transmissible infections observed in the current study is following previous studies among adult populations in different parts of Ghana [10],[11], Africa [1],[2],[16],[18],[24], and the United States [22]. A significant year-on-year decreasing trend of hepatitis B viral infection and HIV was observed in the general population. The trend analysis revealed a reduction in the infection rate from 19.53 per 10,000 in 2015 to 11.70 per 10,000 in 2020 for HBV, and 11.08 per 10,000 in 2016 to 2.81 per 10,000 population at the end of 2020 for HIV (Table 7). In the male population, the cumulative crude prevalence rate for the year-on-year analysis illustrated a similar decreasing trend for both HIV and HBV infection, with the former reducing from a peak in 2016 at 21.8 per 10,000 to the end of 2020 at 5.3 per 10,000 and the latter declining from a peak in 2015 at 39.3 per 10,000 till 2020 at 23.0 per 10,000. On the other hand, the overall infection rate stagnation was observed year-on-year for both HBV and HIV infection among the female populace (Figure 1 and Figure 4). The general decline trend observed for both HBV and HIV infections in this study concurs with the reports by previous authors among asymptomatic adult populations in Ghana [11] and Brazil [25]. On the contrary, the finding of earlier reports by Sajjadi et al. [26] and Yang et al. [27] recorded an upsurge in HBV and HIV infections in Iran and China, respectively. The decreasing trend of HBV and HIV prevalence among the population in the district may reflect the result of periodic screening and vaccination services coordinated by a non-governmental organization (NGO) and other cooperative groups in the region. The change can also be partially attributed to the increasing awareness of HBV and HIV infection in the district as healthcare professionals embark on educational campaigns on the disease throughout the communities in the district for screening. An earlier study posited that decreased incidence of transmittable infections could indicate horizontal transmission correlated with low endemicity, rather than vertical transmission in explaining the possible reasons for the observed phenomenon [16]. In further explanation, Nkrumah et al. [16] asseverated that horizontal transmission is associated to age, socioeconomic conditions, socio-professional status, and dangerous behaviors such as sharing of bath towels, chewing gum, partially eaten candies, or dental cleaning materials, as well as biting fingernails in conjunction with scratching the backs of carriers. In the current study, the 6-year cumulative crude rate and the year-on-year analysis revealed an increasing trend of syphilis infection peaking in 2020 at 33.60 per 10,000 among the general population (Table 7). The surge in the overall crude rate of syphilis infection burden corresponds with the findings of previous reports of Pessoni et al. [25], Lokpo et al. [6], and Bisseye et al. [18]. Of particular importance is the heightened trend of syphilis infection observed among the male populace peaking at 67.3 per 10,000 in 2020. The rate of infection demonstrated a steady flat trend among the female population. The characteristic pattern of syphilis infection in our current study conforms with the finding of the CDC, 2017 report, which revealed an upward trend of syphilis infection and emerging higher cases among males in certain developed states [28]. It is plausible to note that the contributing factors driving the rise in syphilis prevalence were not ostensive in the current study. However, in an attempt of explaining the observed phenomenon, the CDC, in their subsequent report on sexually transmitted diseases surveillance, unraveled that the rise in the rate of reported primary and secondary syphilis infection is primarily attributable to increased cases among men and, specifically, among gay, bisexual, and other men who have sex with men (MSM) which accounted for 53.5% of all syphilis cases [29]. It is essential to note that, although HIV infection has decreased appreciably within the study period, it is cogent to pay critical attention to HIV after observing a rising pattern of syphilis infection because these pathogens are also sexually transmitted, especially syphilis which has lesions that promote transmission of HIV infection [21]. Within the 6-year under review, the year-on-year analysis revealed a dual trend of the overall HCV infection with a decrease from 2016 (6.69 per 10,000) to 2018 (2.02 per 10,000) and an increase till the end of 2020 (6.95 per 10,000 population). A similar dual-trend was depicted among the male gender population, demonstrating a U-shape rate of infection with a single trough in 2018 (2.02 per 10,000) and bimodal infection rates in 2016 (13.5 per 10,000) and 2020 (13.9 per 10,000). In contrast, Walana et al. [11] observed a direct opposite dual trend with an initial increase rate of infection and decreased rate in the final review year during a 3-year study period (2010–2012). The finding of our study suggests that there might be a paucity or ineffectiveness of the strategic management, control, and preventive intervention efforts deployed to combat HCV infection within the district. Also, it might be suggestive of a shift in transmission pathways of HCV infection among the general population. It is well known in literature that age is an independent risk factor for acquiring blood-borne infections [6]. For this reason, one of the objectives of this study is to examine the age difference of the rate of TTIs among the occupants of New Juaben Municipality. Over the past years, previous authors have recorded higher rates of transmittable infections among different age categories, with some observing the highest vulnerability among individuals below 35 years and others reporting higher rates among over 35 year individuals in Africa [30],[31],[32] and Asia [7]. In the present study, it was observed that the rates of all the transmittable infections among the males’ population were more pronounced among persons within the age brackets of 20–29 years revealed by both the crude rate and direct age-standardized rate analysis with rates ranging from 79.79 per 10,000 to 304.50 per 10,000 and from 27.93 per 10,000 to 106.59 per 10,000 population, respectively. In the female population, HBV and HCV infection rates were highly marked among persons within the age brackets of 20–29 years by the crude analysis and after age standardization, the females aged 20–29 years recorded the highest rates of all the infections ranging from 1.58 per 10,000 to 4.03 per 10,000 population. The finding of this study shows that, after standardizing for age, the modal prevalence rate of all the infections were marked among persons between the ages of 20–29 years. This observation compares favorably with the reports of previous studies by Adu-Poku et al. [10] and Pessoni et al. [25], which recorded high TTIs burden among individuals aged between 20 and 29 years in different sub-populations. As emphasized earlier, blood-borne pathogens are also sexually transmitted and associated with engaging in risky behaviors [21]. Therefore, increased incidence of TTIs may suggest rising rates of engaging in risky behaviors among the residents of New Juaben Municipality within the ages of 20 and 29 years.
Our study has some limitations, serological prevalence among repeated and first-time donors could not be ascertained. Furthermore, the study did not include serological prevalence of voluntary non-remunerated blood donors in the municipality. Future studies could be done to examine the crude prevalence both types of blood donors in the community.
Conclusion
The overall burden of transfusion transmissible infections (TTIs) was high among the adult population of the New Juaben Municipality of Eastern Ghana. A prominent gender variation of the infectious burden was observed with male gender preponderance. An increasing trend was recorded for both syphilis and HCV infections. The rates of the infections were highly marked among the youth population within the age brackets of 20–29 years. Therefore, we recommend an appeal to the Ghana Health Service and all other governmental and non-government organizations to maximize and intensify their intervention efforts within the district and target the most vulnerable population to disrupt the transmission chain.
REFERENCES
1.
Keleta YT, Achila OO, Haile AW, et al. Seroprevalence of transfusion transmitted infections among blood donors in Gash Barka Zonal Blood Transfusion Center, Barentu, Eritrea, 2014 through 2017. BMC Hematol 2019;19:5. [CrossRef]
[Pubmed]

2.
Negash M, Ayalew M, Geremew D, Workineh M. Seroprevalence and associated risk factors for HIV, Hepatitis B and C among blood donors in South Gondar District Blood Bank, Northwest Ethiopia. BMC Infect Dis 2019;19(1):430. [CrossRef]
[Pubmed]
3.
Siraj N, Achila OO, Issac J, et al. Seroprevalence of transfusion-transmissible infections among blood donors at National Blood Transfusion Service, Eritrea: A seven-year retrospective study. BMC Infect Dis 2018;18(1):264. [CrossRef]
[Pubmed]
4.
Bisetegen FS, Bekele FB, Ageru TA, Wada FW. Transfusion-transmissible infections among voluntary blood donors at Wolaita Sodo University Teaching Referral Hospital, South Ethiopia. Can J Infect Dis Med Microbiol 2016;2016:8254343. [CrossRef]
[Pubmed]
5.
Buseri FI, Muhibi MA, Jeremiah ZA. Sero-epidemiology of transfusion-transmissible infectious diseases among blood donors in Osogbo, south-west Nigeria. Blood Transfus 2009;7(4):293–9. [CrossRef]
[Pubmed]
6.
Lokpo SY, Dakorah MP, Norgbe GK, et al. The burden and trend of blood-borne pathogens among asymptomatic adult population in Akwatia: A retrospective study at the St. Dominic Hospital, Ghana. J Trop Med 2017;2017:3452513. [CrossRef]
[Pubmed]
7.
Yang S, Jiao D, Liu C, et al. Seroprevalence of human immunodeficiency virus, hepatitis B and C viruses, and Treponema pallidum infections among blood donors at Shiyan, Central China. BMC Infect Dis 2016;16(1):531. [CrossRef]
[Pubmed]
8.
Flichman DM, Blejer JL, Livellara BI, et al. Prevalence and trends of markers of hepatitis B virus, hepatitis C virus and human Immunodeficiency virus in Argentine blood donors. BMC Infect Dis 2014;14:218. [CrossRef]
[Pubmed]
9.
Alomatu H. HIV, HBV, HCV and Syphilis infections among blood donors in Koforidua, Ghana. University of Ghana 2016.
10.
Adu-Poku F, Agboli E, Tarkang EE. Seroprevalence of transfusion-transmissible infections among blood donors in the Hohoe Municipal Hospital, Ghana: 2015–2016: A retrospective hospital-based cross-sectional study. PAMJ - Clinical Medicine 2020;2:12. [CrossRef]
11.
Walana W, Ahiaba S, Hokey P, et al. Sero-prevalence of HIV, HBV and HCV among blood donors in the Kintampo Municipal Hospital, Ghana. Br Microbiol Res J 2014;4(12):1491–9. [CrossRef]
12.
GSS. 2010 Population & Housing Census: District analytical report – New Juaben Municipal 2014.
13.
Osei E, Lokpo SY, Agboli E. Sero-prevalence of hepatitis B infection among blood donors in a secondary care hospital, Ghana (2014): A retrospective analysis. BMC Res Notes 2017;10(1):391. [CrossRef]
[Pubmed]
14.
Tijani A, Silas B, Albert K, et al. Seroprevalence of hepatitis B infection among a population of blood donors in the Kpandai District of Northern Ghana: A five-year retrospective study from 2014 to 2018. J Community Health 2020;45(6):1220–7. [CrossRef]
[Pubmed]
15.
Mremi A, Yahaya JJ, Nyindo M, Mollel E. Transfusiontransmitted infections and associated risk factors at the Northern Zone Blood Transfusion Center in Tanzania: A study of blood donors between 2017 and 2019. PLoS One 2021;16(3):e0249061. [CrossRef]
[Pubmed]
16.
Nkrumah B, Owusu M, Frempong HO, Averu P. Hepatitis B and C viral infections among blood donors. Ghana Med J 2011;45(3):97–100.
[Pubmed]
17.
Nwankwo E, Momodu I, Umar I, Musa B, Adeleke S. Seroprevalence of major blood-borne infections among blood donors in Kano, Nigeria. Turk J Med Sci 2012;42(2):337–41. [CrossRef]
18.
Bisseye C, Mombo LE, Bie SMM, et al. Trends of blood-borne infectious diseases in a rural blood donation center of southeast Gabon (Koula-Moutou). Pan Afr Med J 2018;31:81. [CrossRef]
[Pubmed]
19.
Noubiap JJN, Joko WYA, Nansseu JRN, Tene UG, Siaka C. Sero-epidemiology of human immunodeficiency virus, hepatitis B and C viruses, and syphilis infections among first-time blood donors in Edéa, Cameroon. Int J Infect Dis 2013;17(10):e832–7. [CrossRef]
[Pubmed]
20.
Khedmat H, Alavian SM, Miri SM, et al. Trends in seroprevalence of Hepatitis B, Hepatitis C, HIV, and Syphilis infections in iranian blood donors from 2003 to 2005. Hepat Mon 2009;9(1):24–8.
21.
Mohammadali F, Pourfathollah AA. Changes in frequency of HBV, HCV, HIV and syphilis infections among blood donors in Tehran province 2005–2011. Arch Iran Med 2014;17(9):613–20.
[Pubmed]
22.
Steele WR, Dodd RY, Notari EP, et al. Prevalence of human immunodeficiency virus, hepatitis B virus, and hepatitis C virus in United States blood donations, 2015 to 2019: The Transfusion-Transmissible Infections Monitoring System (TTIMS). Transfusion 2020;60(10):2327–39. [CrossRef]
[Pubmed]
23.
Dongdem JT, Kampo S, Soyiri IN, Asebga PN, Ziem JB, Sagoe K. Prevalence of hepatitis B virus infection among blood donors at the Tamale Teaching Hospital, Ghana (2009). BMC Res Notes 2012;5:115. [CrossRef]
[Pubmed]
24.
Nada HA, Atwa M. Seroprevalence of HBV, HCV, HIV and syphilis markers among blood donors at Suez Canal University Hospital Blood Bank. J Blood Disord Transfus 2013;5(1):1–5.
25.
Pessoni LL, de Aquino ÉC, de Alcântara KC. Prevalence and trends in transfusion-transmissible infections among blood donors in Brazil from 2010 to 2016. Hematol Transfus Cell Ther 2019;41(4):310–5. [CrossRef]
26.
Sajjadi SM, Pourfathollah AA, Mohammadi S, Nouri B, Hassanzadeh R, Rad F. The prevalence and trends of Hepatitis B, Hepatitis C, and HIV among voluntary blood donors in Kohgiluyeh and Boyer-Ahmad Transfusion Center, Southwestern Iran. Iran J Public Health 2018;47(7):944–51.
[Pubmed]
27.
Yang Y, Guo C, Liu L, Zhang T, Liu W. Seasonality impact on the transmission dynamics of tuberculosis. Comput Math Methods Med 2016;2016:8713924. [CrossRef]
[Pubmed]
28.
CDC. Sexually Transmitted Disease Surveillance 2018.
29.
de Voux A, Kidd S, Grey JA, Rosenberg ES, Gift TL. State-specific rates of primary and secondary syphilis among men who have sex with men — United States, 2015. MMWR Morb Mortal Wkly Rep 2017;66(13):349–54. [CrossRef]
[Pubmed]
30.
Bartonjo G, Oundo J, Ng’ang’a Z. Prevalence and associated risk factors of transfusion transmissible infections among blood donors at Regional Blood Transfusion Center Nakuru and Tenwek Mission Hospital, Kenya. Pan Afr Med J 2019;34:31. [CrossRef]
[Pubmed]
31.
Biadgo B, Shiferaw E, Woldu B, Alene KA, Melku M. Transfusion-transmissible viral infections among blood donors at the North Gondar district blood bank, northwest Ethiopia: A three year retrospective study. PLoS One 2017;12(7):e0180416. [CrossRef]
[Pubmed]
32.
Chama D, Ahmed Y, Baboo KS, Halwindi H, Mulenga J. Transfusion transmissible infections among voluntary blood donors at the University Teaching Hospital, Lusaka, Zambia. Medical Journal of Zambia 2015;42(3):90–5.
SUPPORTING INFORMATION
Acknowledgments
We wish to acknowledge staff of the Eastern Regional Hospital Blood Bank and the Laboratory for their invaluable contribution toward this study.
Author ContributionsFrancis Abeku Ussher - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Osmanu Taufik - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
James Osei-Yeboah - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sylvester Yao Lokpo - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
George Damptey Danquah - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
George Kwasi Kwakye - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Joyce Der - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Francis Abeku Ussher et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}